
 Photo: Sensimed
Photo: Sensimed
Poets say the eyes are a window to the soul. But biomedical engineers are using the eyes to gain insight into the body.
They’re hard at work on futuristic-sounding technology that uses smart contact lenses and implantable lenses to diagnose, monitor, and treat a wide range of diseases. In 2014, two of the largest multinational companies made an announcement that brought this new technology into sharp focus. Google, through its biology offshoot, now named Verily Life Sciences, and the Swiss pharmaceutical giant Novartis International, through its eye care division Alcon, joined forces to design, develop, and commercialize smart contact lenses for diabetics. If the project reaches its goals, these lenses will spare diabetics from the daily finger pricks typically used to measure blood glucose levels, instead employing embedded microelectronics to measure glucose in the wearer’s tears.
Verily and Alcon aren’t the only ones pushing smart-lens technology forward. In labs around the world, biomedical engineers have been making exciting progress on smart lenses to diagnose diseases and allow unobtrusive and continuous monitoring of patients. In fact, two smart-lens products have already hit the market in Europe to help patients with glaucoma, one of the world’s most common eye diseases.
All of the efforts rely on two basic types of smart lenses: contact lenses similar to those used for vision correction and intraocular lenses that must be surgically implanted in the eye. The former are obviously easier to put into position, as they can be slipped into the eye on a fingertip. They also allow for a broader range of physical and biochemical microsensors, because the lenses can be replaced when the sensors wear out. Intraocular lenses, on the other hand, allow for long-term monitoring without the patient having to take any action.
Both types of lenses may benefit from new kinds of flexible electronics that are microscopic or semitransparent. Advances in materials science have also made it possible to fabricate lenses from materials like hydrogels, which can tolerate the physical stress of eye movements while allowing oxygen to pass through and nourish the eye. Although significant technical challenges remain, we’re already beginning to look into people’s eyes—not for emotional revelations but for medical ones.
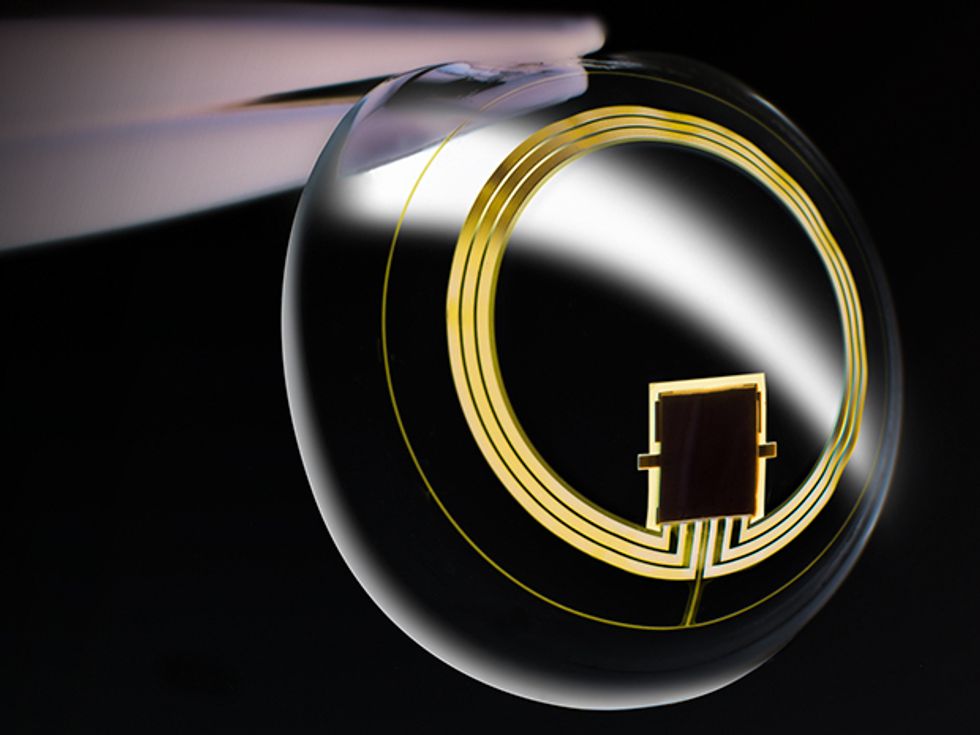
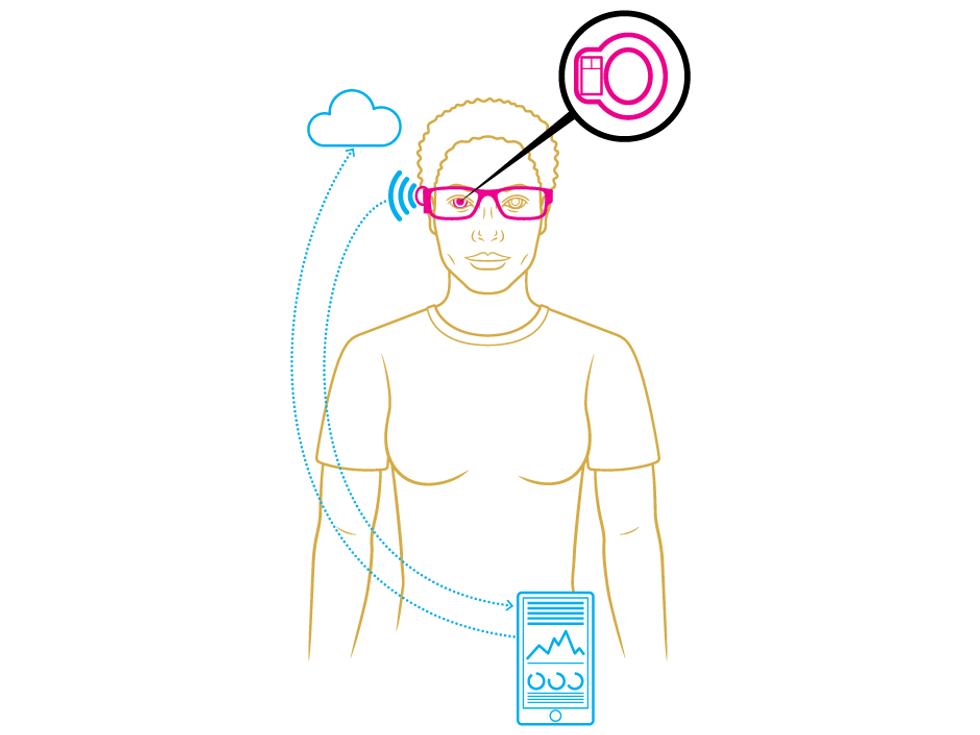
 Golden Eye: The Triggerfish smart contact lens for glaucoma monitoring uses an antenna made of gold to both receive power and send out data.Photo: Sensimed
Golden Eye: The Triggerfish smart contact lens for glaucoma monitoring uses an antenna made of gold to both receive power and send out data.Photo: Sensimed
To fit comfortably in or on the eye, a smart lens must measure about 14 millimeters in diameter and a mere 100 to 200 micrometers thick. That small curved disk must incorporate sensors as well as microelectronics to manage power consumption, control the sensors’ operations, and transmit the sensors’ readings to an external device such as a smartphone. In these tiny lenses, the biggest challenges are supplying power and ensuring that the sensors give reliable readings.
Powering a thin piece of instrumented plastic pressed against a human eyeball isn’t an easy task. Conventional batteries are much too big, and their packaging would have to be reengineered to ensure that any leaking chemicals wouldn’t harm the wearer. Wireless power transfer is therefore more appealing. Its main drawback is that the source of power must be very close to the lens—typically just a few centimeters. To discreetly solve this problem, some experimental systems (including those developed in my lab at the University of Applied Sciences of Southern Switzerland) embed the power transmitter in eyeglass frames.
The most convenient way to transmit wireless power is near-field inductive coupling, the same method used to charge electric toothbrushes in their base stations and smartphones on the charging pads at Starbucks. For smart lenses, the transmitting coil can be placed in the eyeglasses, and the receiving coil is embedded near the lens’s outer border. Near-field inductive coupling operates at low frequencies, typically a few megahertz, so the transmission poses no threat to the eye tissue. Some labs have experimented with far-field inductive coupling, beaming power to the lens via microwaves, but these systems operate at higher frequencies (typically a few gigahertz) and require precautions to avoid damaging eye tissue.
A more futuristic approach is to have the lenses power themselves. At Ghent University, in Belgium, Herbert de Smet’s lab has inserted miniature photovoltaic cells into lenses to collect solar power. Other researchers are exploring how to use piezoelectric elements to turn the vibrations caused by eye movements into electrical power; Samsung, for example, recently applied for a patent on a piezoelectric smart lens. Another far-out idea uses fuel cells that convert chemicals present in human tears into electricity. Of course, it will be some time before any of these in situ power technologies is ready for real-world use.
Designing biosensors for smart lenses poses another challenge. Smart contact lenses need highly accurate sensors that can be manufactured cheaply (particularly if the lenses are disposable), while smart intraocular lenses need sensors that will keep working in the eye for at least 10 years to avoid repeated surgery. Biosensors that rely on an enzymatic reaction to detect biomarkers like glucose or lactate in the eye’s fluids don’t last long, because such sensors’ enzyme activity declines over time. Some research groups are therefore working on biosensors on the nanoscale, so that hundreds or even thousands of sensors could be embedded in one lens, thereby increasing the lens’s longevity. Eventually, nanosensors could be made sensitive enough to detect a single molecule of the target chemical; the diameter of a graphene-silver nanowire, for instance, is comparable to the size of a glucose molecule.
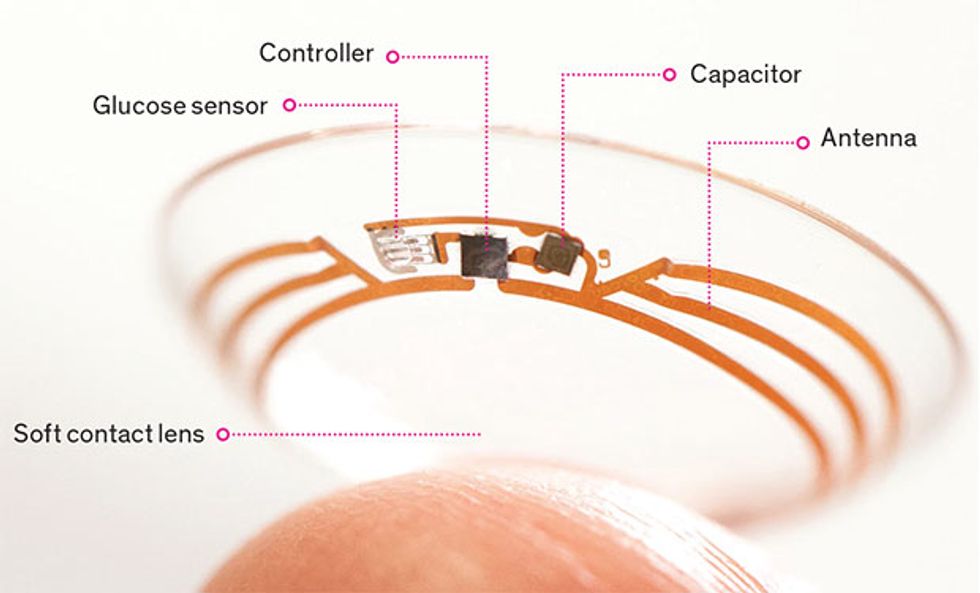 Telltale Tears: This diabetes-monitoring contact lens, still under development by researchers at Google and Novartis, measures glucose levels in the wearer’s eye fluids.Photo: Verily Life Sciences
Telltale Tears: This diabetes-monitoring contact lens, still under development by researchers at Google and Novartis, measures glucose levels in the wearer’s eye fluids.Photo: Verily Life Sciences
For the 422 million people worldwide who have diabetes, a smart contact lens with a microsensor that continuously measures glucose levels could be a life-changing technology. Today, most diabetics monitor the glucose in their blood by pricking their fingers many times each day—a necessity because the level of glucose fluctuates in response to meals, exercise, and other common activities. Even continuous glucose monitors, which use electrodes that sit under the skin, require multiple daily finger pricks for calibration. When Google announced its smart-lens project in 2014, the project leads noted that some diabetics compare managing their glucose levels to “having a part-time job.”
Contact lenses offer a view into the interior of the body via the fluids that bathe the eye. For monitoring diabetes, most smart lenses use sensors that measure the glucose concentration in basal tears, the fluid that lubricates the cornea and washes it clean of dust.
Many types of sensors have been developed for measuring the glucose in these tears. The best known is the electrochemical sensor devised by Babak Parviz while he was an electrical engineering professor at the University of Washington; he later became a director at Google and launched the Verily-Alcon smart-lens project. This sensor uses an enzyme that catalyzes glucose to create hydrogen peroxide, which is further oxidized at the electrode to release electrons, thus generating an electrical current proportional to the glucose concentration.
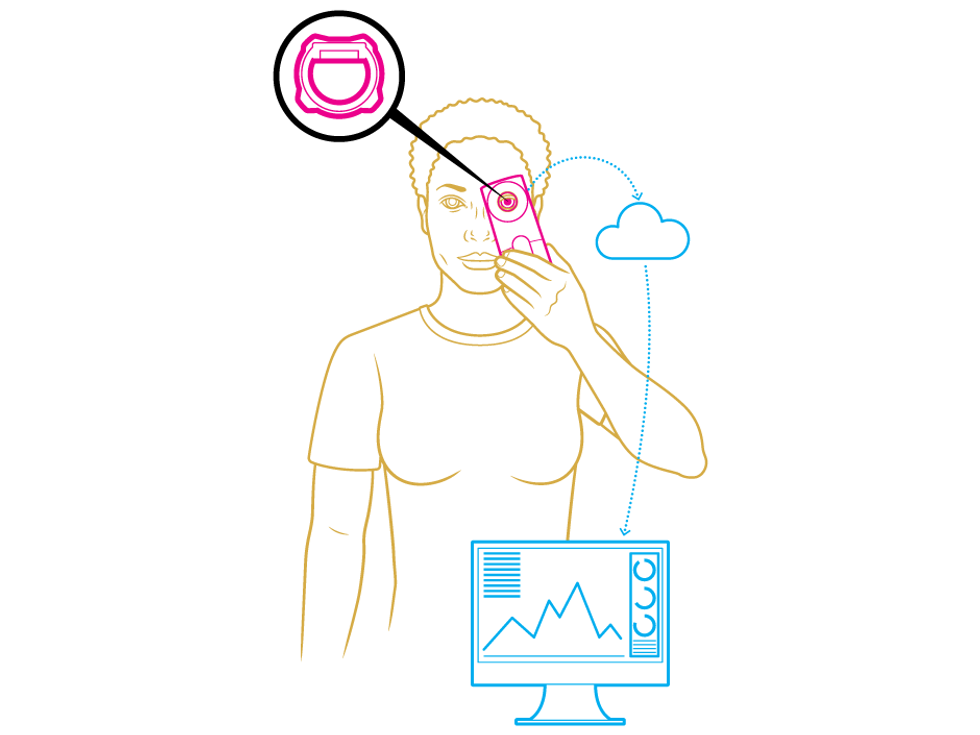
Other types of sensors use fluorescent or colloidal-crystal particles to provide an optical readout that indicates the amount of glucose present. For example, users could look in the mirror to check the color of tiny dots on their smart lenses.
Before any of these technologies can turn into commercial products, researchers still have to answer several scientific questions. The first relates to the minute amount of glucose found in basal tears: Typical tear glucose levels are on the order of 0.1 to 0.6 millimole, while glucose levels in the blood range from about 4 to 6 mmol. Some researchers therefore argue that tears simply don’t contain enough information to be useful for diabetes monitoring. Others counter by citing studies that examined tears using mass spectrometry, the gold standard of analytical chemistry, and found that glucose is present at low but consistent levels. Unfortunately, it’s impossible to pack a mass spectrometer onto a smart lens, and biochemical sensors can’t match the accuracy of mass spectrometry.
Scientists are also debating the correlation between glucose levels in blood and those in tears. Animal studies have shown an average lag time of 13 minutes between a rise or fall in blood glucose level and when such a change shows up in tears. If such a delay is consistent, it could be taken into account during the calibration of smart-lens systems. However, if the time lag varies, it will be very difficult to create tear-monitoring systems that diabetics can rely on.
And then there’s the question of the chemical composition of the three different types of tears: the basal tears that lubricate the eye, the tears caused by eye irritation, and the heartfelt tears that spring from emotions. Is the amount of glucose significantly different in these three fluids? If so, users’ glucose readings could spike or dip whenever they started to cry or got a speck in their eye.
Despite these open questions, smart contact lenses have great potential for medical monitoring. Already, researchers are looking at substances other than glucose that are found in the eye and might be used to diagnose other disorders. For example, lactate in tears could be an early warning of sepsis, an acute infection that’s a common killer in hospitals.
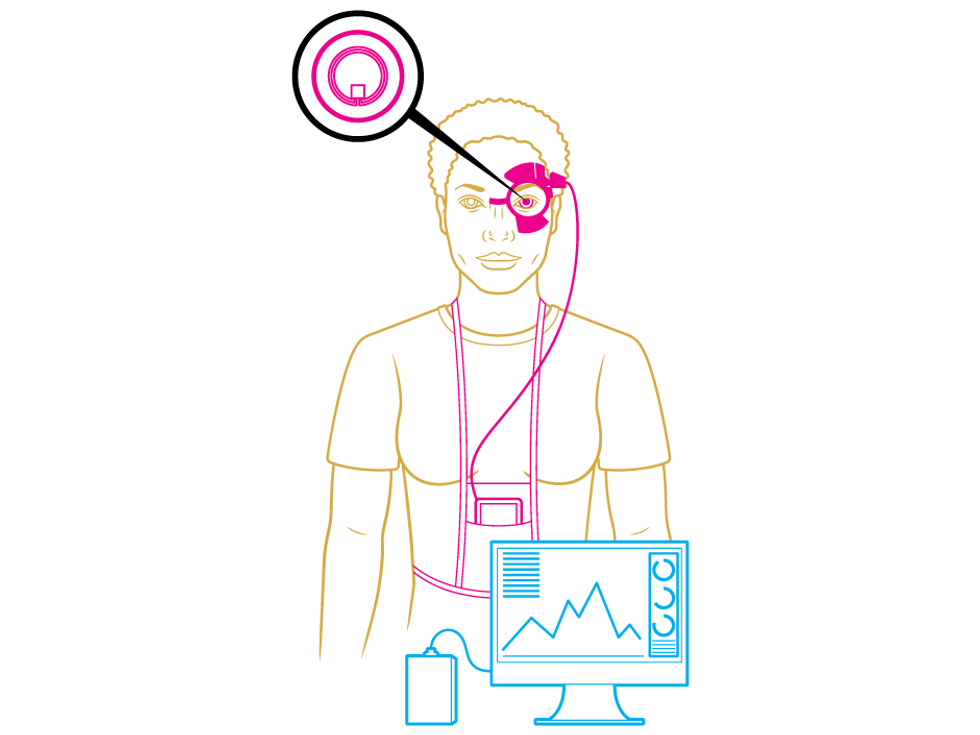
To diagnose and monitor glaucoma, three different varieties of smart lens can record intraocular pressure. The Triggerfish contact lens transmits information to an adhesive patch that’s connected to a recording device. After 24 hours of wear, the user returns to the eye doctor.
A person suffering from glaucoma typically loses peripheral vision first, and the darkness gradually creeps inward. Glaucoma afflicts 67 million people worldwide, and it’s the leading cause of irreversible vision loss and blindness. The first two smart-lens products to reach the commercial market are a contact lens and an implanted lens to help patients with this devastating disease.
Doctors know that the biggest risk factor for glaucoma is high intraocular pressure (IOP), which damages the optic nerve. Today, ophthalmologists measure IOP during eye exams using tools called tonometers, which either send a puff of air into the eye or press a probe against the eye’s numbed surface. Monitoring a patient’s eye pressure over time requires repeated office visits, an inconvenience that prevents some people from managing their illness effectively.
Smart lenses could do better because they continuously measure IOP using embedded sensors. The IOP of a healthy human eye is between 1,300 and 2,800 pascals, whereas in a diseased eye the pressure can range from 500 to 6,500 Pa. What’s more, an individual’s IOP fluctuates with their circadian rhythm—with the highest pressure typically occurring at night while the person is lying in bed. Getting 24 hours’ worth of IOP readings is valuable to eye doctors because it yields the patient’s true IOP profile.
The commercial contact lens for glaucoma comes from the biotech company Sensimed, based in Lausanne, Switzerland. Its Triggerfish lens, already available in 33 countries, recently gained regulatory approval for use in the United States. The soft disposable lens uses piezoresistive strain sensors to measure IOP. The sensors detect the slight change in the circumference of the cornea when it stretches due to fluid pressing on it from behind. Pressure readings are taken every 5 minutes over a 24-hour period, and the lens transmits the data wirelessly, using near-field induction, to a receiver placed in an adhesive patch that encircles the user’s eye. A wire connects the receiver to a recording device that the patient wears in a pouch hung around the neck.
Doctors are using Sensimed’s device to diagnose patients at risk of developing glaucoma, as well as for existing glaucoma patients, giving them periodic checkups to track the progress of the disease. For now, that’s where the utility of the Triggerfish lens ends; the system is too cumbersome for long-term wear.
The first commercial smart lens for implantation in the eye comes from Implandata Ophthalmic Products, of Hannover, Germany, which received regulatory approval in Europe for its Eyemate lens in May 2017. While a lens that requires surgical implantation may not seem as convenient as a disposable lens, the surgery isn’t a major drawback. The implantation can be done during routine cataract surgery, a quick outpatient procedure that millions of people undergo every year. In cataract surgery, a tiny incision is made in the eye, and the cataract-clouded lens is removed and replaced by an artificial intraocular lens; this lens sits behind the colored ring of the iris, so it’s not visible. For glaucoma patients, the surgeon can instead insert the Eyemate intraocular lens, with its embedded pressure sensor and accompanying microelectronics. Patients will go home with a handheld device that they’ll regularly hold up to their eye to collect recorded IOP data and power the lens via inductive coupling.
Even so, why bother with surgery when smart contact lenses are so much easier to deal with? The most obvious reason is that an implanted lens can provide long-term monitoring, not just a 24-hour checkup. The other reason is accuracy: One disadvantage of the Triggerfish contact lens is that it determines pressure indirectly, by measuring cornea deformation and then correlating that data to an IOP value. This correlation step introduces errors. By contrast, the Eyemate intraocular lens directly measures IOP and yields more accurate data. Its eight tiny pressure sensors resemble plate capacitors. Each sensor has a rigid plate and a flexible membrane, and when the membrane is pushed closer to the plate by the pressure in the eye the overall capacitance changes, generating an analog signal that’s changed to a digital signal on the chip.
In my lab, we’ve long been experimenting with smart intraocular lenses for both glaucoma monitoring and other applications. Our glaucoma lens directly measures IOP using piezoresistive strain sensors; these sensors contain electrical conductors that stretch under pressure, thus changing their resistance and providing a readout of IOP. We’ve also used an implanted lens to monitor glucose concentrations in the aqueous humor—the fluid that fills a chamber behind the cornea—but the biochemical microsensors we’ve tried haven’t lasted long enough to be practical for long-term use.
While the technological and scientific challenges of smart contact and intraocular lenses are significant, the lenses’ potential for disease diagnosis and monitoring guarantees that work will continue. In the next decade, you can expect to see the commercial introduction of a wide range of smart lenses for medical applications. Meanwhile, researchers around the world continue to investigate new biomarkers in tears, develop new energy-harvesting and storage technologies, fabricate new types of flexible electronic devices, and construct more reliable biosensors. Other researchers are designing lenses to treat disease, with microfluidic components that deliver drugs on command. With these new technologies, we’ll have a better view of human biology than ever before.
This article appears in the August 2017 print issue as “Look Into My Eyes.”
About the Author
Diego Barrettinorecently moved to the Lucerne University of Applied Sciences and Arts from the University of Applied Sciences of Southern Switzerland, where he continues his work on smart contact lenses and eye implants.