
Breast cancer remains a leading cause of cancer deaths among women in many parts of the world. But better diagnosis and treatment of it has noticeably improved the outcome of the disease, reducing death rates over the last decade by about 2 percent per year in the United States, according to the U.S. Institute of Medicine, Washington, D.C. Part of that success is owed to earlier detection by the standard breast imaging technology, film-screen X-ray mammography.
Source: U.S. Institute of Medicine
Click on the image to enlarge.
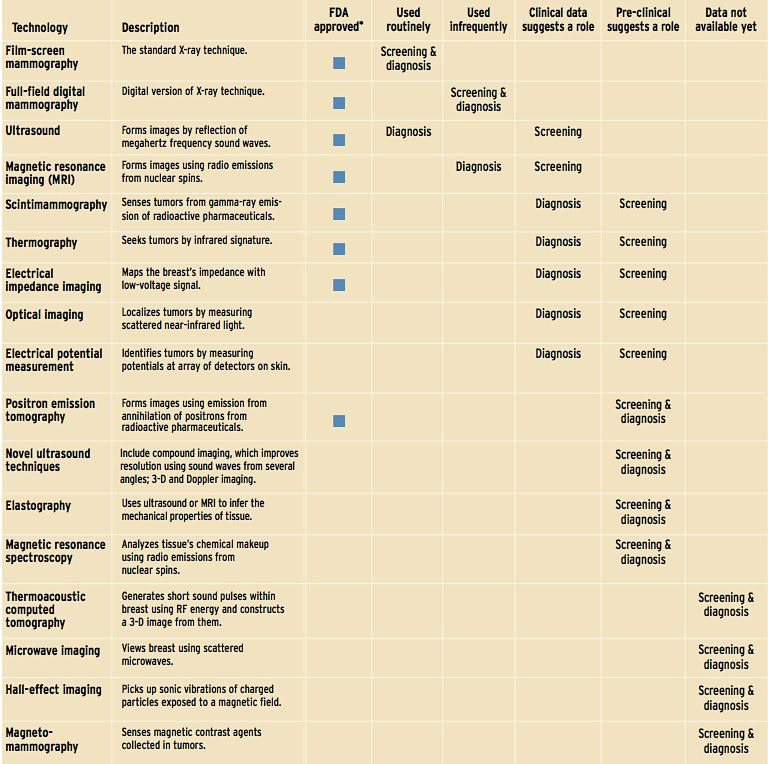
But the variety and sophistication of alternative imaging technologies in development have increased greatly to encompass everything from optical laser imaging to digital mammography [see "Imaging Technologies for Breast Cancer," right]. While these new technologies have shown impressive results, a report released in March by the Institute of Medicine concludes that they will be playing only a supporting role to film-screen mammography, for some time to come.
"Although many of the newer tools offer certain advantages and deserve to be studied further, film mammography remains the gold standard for screening against which new imaging technologies must be measured," said Dr. Joyce Lashof, chair of the Institute of Medicine committee that authored the report. Technologies ultimately intended for screening are likely to work their way toward proving themselves as adjuncts for screening or diagnosis, giving additional information on breast abnormalities seen in mammograms or spying them in breasts too difficult to analyze with X-rays.
As it stands now, abnormalities, or lesions, are discovered either by physical examination or by a screening mammogram read by a radiologist. Once identified, the abnormality must be diagnosed as benign or malignant by using other imaging technologies such as ultrasound or a biopsy and microscopic examination. Finally, tumors are biochemically characterized and categorized, or staged, according to their size and how much they have spread. The system has its flaws, though. It misses up to 20 percent of lesions, and many of those found turn out to be benign. In all three steps—examination, diagnosis, and categorization—new imaging technologies could help.
SENSITIVITY: a measure of how often a test correctly identifies women with breast cancer. It answers the question: if the disease is present, how likely is the patient to have a positive test?
SPECIFICITY: a measure of how often a test correctly identifies a woman as not having breast cancer. It answers the question: if the disease is absent, how likely is the patient to have a negative test?
But the Institute of Medicine, one of the U.S. National Academies, expressed concern that as new technologies are approved for diagnosis, they might be prematurely adopted for screening. The two roles are quite different. Screening tools are applied first: they need to be highly sensitive, identifying as correctly as possible women who have breast cancer. Then, diagnostic tests are used on the women identified to determine if they really do have cancer, what type it is, and how far it has spread. Diagnostic tools must have high "specificity"—according to the medical terminology—correctly weeding out women who do not have cancer [see "Defining Terms," right].
After surveying the medical-imaging field, Lashof and her colleagues concluded that, so far, no single imaging method has both high sensitivity and high specificity for breast cancer. Still, scientists and engineers are making some progress. X-ray equipment makers have digital machines in various stages of development, software to help radiologists find tumors on mammograms is available, and scientists have researched such novel techniques as enzymatically activated contrast agents.
X-rays go digital
Digital mammography is the new technology most certain to see clinical use, but it has been a long time coming. With its high spatial and contrast resolution requirements, mammography demands very small pixels and a high signal-to-noise ratio. "Mammography is clearly the most challenging of the imaging technologies," said Roman Janer, vice president of breast imaging at digital X-ray machine maker Hologic, in Bedford, Mass.

he digital version of the technology has superior dynamic range and linearity compared to film, leading to better contrast resolution. It allows the images to be manipulated and analyzed with software [see photo]. This combination may lead to the discovery of more subtle features indicative of cancer and to a greater ability to distinguish between potential cancers and harmless tissue abnormalities.
The evidence to date is weak on the former issue but stronger on the latter. Dr. John M. Lewin, assistant professor of radiology at the University of Colorado Health Sciences Center, in Boulder, and colleagues could not see a significant difference in the number of cancers detected using film mammography or a digital mammography machine developed by General Electric Co. But the doctors noted that fewer women needed to be called back for follow-up tests with the GE device—indicating that there were fewer false-positives. To obtain a broader perspective on digital mammography's merits, a 40 000-woman trial, testing several kinds of digital detectors, is under way by the American College of Radiology Imaging Network in Philadelphia.
Several companies, including Fuji Photo Film, GE, and Siemens, have digital mammography systems in development. The technologies they use for making digital images can be broadly placed into two classes: indirect detection, or scintillator X-ray conversion, and direct detection, or electronic X-ray conversion. In indirect detection, X-rays are converted into visible light and then picked up on a solid-state detector. Direct detection, a more advanced technique aiming for higher resolution, converts X-rays directly into electric signals.
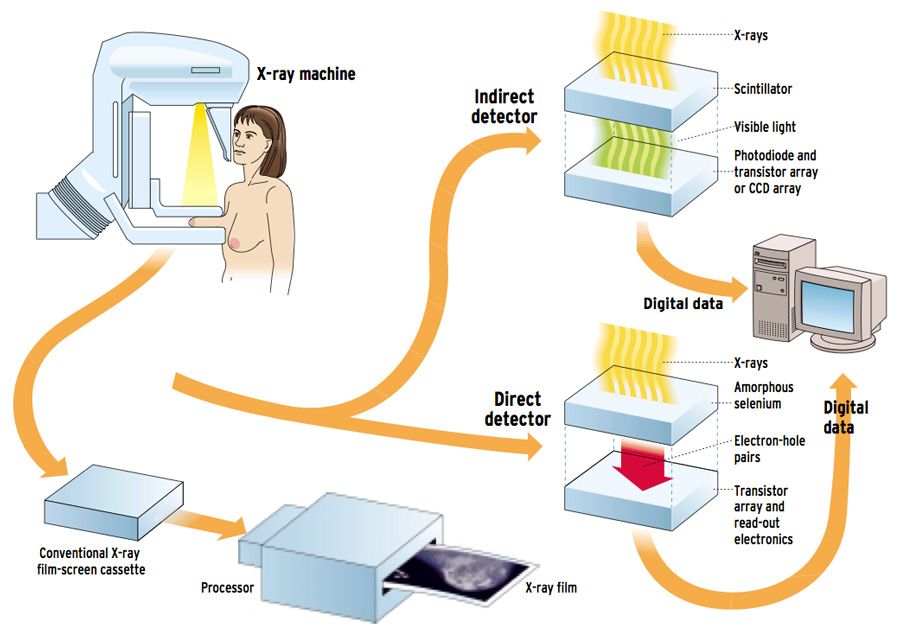
Currently, the only company to gain approval for its digital equipment from the U.S. Food and Drug Administration (FDA), Rockville, Md., is GE Medical Systems in Waukesha, Wis., and it uses the indirect approach. With indirect detection, X-rays pass through the breast and then strike a scintillator, a material that absorbs the X-rays and emits visible light. The scintillator is coupled to a photodetector array or connected to tiles of charge-coupled devices (CCDs) by tapered optical fibers [see illustration]. GE uses needle-like crystals of cesium iodide as a scintillator and an amorphous silicon detector made up of photodiodes and thin-film transistor (TFT) readout circuitry.
GE designed its detector with a higher degree of speed and sensitivity, termed detective quantum efficiency, than is needed for mammography alone, Scott Schubert, the company's manager of global X-ray R&D, told IEEE Spectrum. Because the higher sensitivity allows for lower doses of X-rays, those better-than-need-be characteristics may allow for the detector's use in breast tomosynthesis—a method of constructing three-dimensional images from scans taken at several angles. With 3-D imaging, greater knowledge of a lesion's nature and location may be gained. "Tomosynthesis needs to take 11 images over 3 to 5 seconds," said Schubert. But all 11 images must be taken using a total dosage of radiation equal to one standard film mammogram.
Competing with GE's tool in two-dimensional mammography is one from Fischer Imaging Corp., Denver, Colo. Fischer's detector uses CCDs in its indirect architecture. But rather than image the breast in one shot, the machine scans a narrow slot of collimated X-ray beams across the breast. In conventional mammography, X-rays that scatter off breast tissue create a contrast-reducing haze on an image if they are not first screened out with a grid placed between the breast and the film or detector. Fischer's slot-scanning technique eliminates the need for a grid, because the slot of the exposed detector is so narrow that scattered X-rays fall outside it. "The slot technique fundamentally results in a lower dosage of X-rays because there is no grid to absorb photons," claimed Ken Crocker, director of marketing at Fischer.
An important design consideration in making indirect detectors is choosing the thickness of the scintillator, said Hologic's Janer. A thicker scintillator captures more X-rays, but also leads to a loss of resolution because the photons have more chance to scatter before reaching a CCD or photodiode.
Hologic and others are now researching direct detection, a way to dodge the scintillator-thickness design constraint entirely. Direct detection omits the conversion of X-rays to visible light, thus removing the loss from scattering of that light.
Hologic is targeting its device to begin limited testing in July. In designing the device, the company replaced its original CCD-based indirect system with an amorphous silicon TFT array coated in amorphous selenium. A voltage is placed across the selenium, and wherever an X-ray strikes it, electron-hole pairs are formed. These pairs are then collected by integrated capacitors associated with the pixel elements of the TFT array, and the image is read out by electronics integrated in the array.
Though digital mammography has yet to prove itself any better at spotting early signs of cancer than film mammography, having digital files, rather than stacks of film, will let hospitals and mammography clinics store and transfer information more easily. Also, developers are hoping image enhancement and other software-based techniques will add enough functionality for radiologists to see an improvement.
The other CAD
As with many labor-intensive occupations, radiologists now also have an automated helpmate: computer-aided detection (CAD) systems that can identify potential cancers on mammography images. These software systems are entering clinical practice as a way to improve radiologists' ability to detect the few cancer cases in the sea of normal-looking images they see every day. In a typical screening situation, a mammographer will uncover only 1.5-6 cancers for every 1000 films he or she reads. Some cancers are inevitably overlooked, but having two radiologists looking at each film has been shown to improve the detection rate by as much as 15 percent, according to studies cited in the Institute of Medicine report. So academic researchers and a few companies have been developing CAD as an artificial second radiologist.
The first to gain FDA approval for a CAD tool targeted to breast cancers was R2 Technology Inc., in Los Altos, Calif. But others such as CADx Medical Systems, in Laval, Que., Canada, and Scanis Inc., Foster City, Calif., are also developing products.
To use CAD, conventional X-ray films must first be digitized. After that step, the software processes the digital image to improve the contrast between potential problem areas and the background. It then picks out all the potential lesions in an image—homing in on suspected masses and clusters of microcalcifications, which are flecks of calcium often associated with tumors. The software completes its operation by throwing out false positives using neural network, statistical learning, or other types of algorithms that can be optimized through training [see photo].
CAD software must be trained on hundreds of X-ray mammograms with cancerous lesions. But a big problem for CAD developers inventing new detection algorithms is gaining access to so large a number of films. "[Training] databases are extremely expensive to generate," said Steve K. Rogers, president and chief executive officer of Qualia Computing Inc., in Beavercreek, Ohio, the company that is developing the CAD system manufactured and distributed by CADx. Rogers' company and R2 Technology separately gathered thousands of mammography films on which to train their software. On top of that, before the FDA will approve any new software, the companies have to try out their systems on thousands of additional patients to guarantee their efficacy.
Because digital mammography equipment is new to the market, no substantial databases exist for digitally acquired mammograms. So companies are hoping their software will be able to smooth over any differences in resolution between digitized film and digitally acquired images, as well as between images acquired using different digital detectors.
In one promising approach, Jimmy Roehrig, R2 Technology's chief scientific officer, told Spectrum that his company has developed a way to map the characteristics of GE's detector to those of digitized film, in this way making the one equivalent to the other for the purposes of the detection algorithms. This strategy avoids a more fundamental change to the software, such as retraining the neural network.
Similarly, R2's competitor, Qualia Computing, advocates "plug and play" CAD that will be able to operate on images from different detectors as well as on digitized film. To date, the company has built software to normalize three digital detectors to match the characteristics of digitized film.
More than mammograms
Other well-established imaging technologies, such as magnetic resonance imaging (MRI), positron emission tomography (PET), and ultrasound, are in various stages of use—not in screening, but in diagnosis, helping to clarify the nature of suspicious objects seen on mammograms. For instance, physicians frequently use ultrasound to help determine whether a lesion detected on a mammogram is a malignant mass or a harmless cyst.
Despite the diagnostic support they offer, each of these technologies has its limitations. MRI's specificity is highly variable, ranging from 28 to 100 percent, depending on the interpretation technique used and the patient population; PET scanners are expensive and scarce, and ultrasound has trouble seeing microcalcifications because of so-called speckle—tiny bright flecks on the image caused by scattered echoes.
Technical fixes are in the works, nonetheless. In ultrasound, for example, ATL Ultrasound of Bothell, Wash., an affiliate of Philips Medical Systems North America, in Shelton, Conn., has found a way to eliminate speckle and improve image contrast in general by reflecting sound off tissue from multiple angles. The device directs the ultrasound beam at nine angles sequentially, then reconstructs the image from all those viewpoints in real time.
Plugging into biochemistry
Since imaging principally relies on the physical characteristics of a cancer, such as its relative opacity to different wavelengths of light, it alone may not have all the answers. But if an imaging technique is combined with knowledge of the biological and biochemical nature of cancer, both sensitivity and specificity might be improved.
One company looking to make that combination is Imaging Diagnostics Systems Inc., in Plantation, Fla. The firm makes a breast imager that uses an optical wavelength laser instead of an X-ray source and computes the image from scattered, rather than transmitted, photons. It presents a 3-D picture of breast anatomy that Richard Grable, the company's CEO, hopes will be adopted as a diagnostic tool.
But in order to move optical imaging from diagnosis to screening, the technology must use contrast agents that take advantage of what is known about tumor biochemistry, according to Grable. His company is working with pharmaceutical firms, which he would not name, on developing compounds that will bind specifically to tumors. Then, shine the laser through the breast, and the tumors would be seen to fluoresce.
Along those same lines, a team led by Britton Chance, emeritus professor of biochemistry and biophysics at the University of Pennsylvania School of Medicine, in Philadelphia, and an optical imaging pioneer, has invented an optical "beacon" that makes cancer cells shine 20 times as bright as normal tissues. First, fluorescent molecules, encapsulated in a specific protein coating, are injected into the bloodstream. When enzymes within the tumor open the capsule, the beacon molecule is unveiled. If the beacon is struck by light from a laser, it fluoresces brightly enough to be detected at the skin surface.
MRI may make use of a similar technique to capture a better image. A tumor-specific contrast agent, developed by Thomas Meade at the California Institute of Technology, in Pasadena, Calif., relies on the element gadolinium to exert a strong influence on the magnetic moment of the hydrogen protons in water—the dominant signal in MRI. In Meade's technique, a gadolinium atom is bound up in a macromolecule and capped with a compound that is removed by an enzyme within the tumor. The exposed gadolinium interacts with nearby protons, creating a highly localized signal. "[The resolution of] traditional MRI is in the millimeter regime," Meade said. "To track cells, you need micrometer resolution, which we can achieve with this technique."
Obstacles in development
The road to developing a new technology to the point of clinical usefulness and then getting it broadly adopted is long and difficult, the institute's committee noted.
The scientific hurdles could be lowered. Among the institute's recommendations is that the U.S. National Cancer Institute, in Bethesda, Md., establish a permanent infrastructure for testing new detection technologies as they emerge. That infrastructure might include databases and archives of clinical samples. The institute also urged a streamlining of the process for gaining government reimbursement and FDA approval for new technologies. In particular, the committee proposed that conditional reimbursement be granted for a diagnostic technology whose developers wished to pursue a large-scale screening trial, so that the technology could be assessed more quickly.
Economic obstacles loom large as well. New technologies like digital mammography are not cheap. A digital machine weighs in at $400 000-$600 000 compared to a film-based device at $50 000-$70 000. Also, reimbursement by U.S. insurers to physicians is low, ranging from $35 to $75 per patient, which is less than cost. "The rest of the department sees [mammography] as something they ought to do—kind of like eating your vegetables,"said Dr. Etta Pisano, professor of radiology and chief of breast imaging at the University of North Carolina School of Medicine in Chapel Hill.
Additional reporting by Steve Miller
To Probe Further
For more background on the U.S. Institute of Medicine's findings on early detection of breast cancer, see the report, "Mammography and Beyond: Developing Technologies for the Early Detection of Breast Cancer," published by the National Academy Press, Washington, D.C. The document includes the institute's full recommendations and evaluation of technologies and public policies. It is available free of charge on the Web at https://national-academies.org/webextra/brcancer.
Information on how the U.S. Food and Drug Administration regulates mammography may be obtained at https://www.fda.gov/cdrh/mammography.
A good Web site that links to a number of digital mammography and computer-aided detection research groups, as well as to several companies involved in providing mammography equipment, has a Web address of https://www.rose.brandeis.edu/users/mammo/digital.html
Comprehensive statistics on breast cancer mortality are assembled in "Global Breast Cancer Mortality Statistics," in CA Cancer Journal for Clinicians, Vol. 49, pp. 138-44. The publication may be obtained for a small fee through the American Cancer Society at https://www.cancer.org.